1801006064 SHORT CASE
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 38 year old male , who is a civil engineer by profession and resident of West Bengal came to OPD with chief complaints of :
Abdominal pain since 5years
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 5 years ago then he developed abdominal pain which was sudden in onset and progressive in nature.
Pain occured once in every 3 months in the past 41/2 years but since 6 months he is having pain once in a month.pain is radiating to the back and dragging type of pain.
It aggravates on taking alcohol and relieved on medication.
Since 1 year he had episodes of vomiting which was non bilious ,non projectile and water as content followed by abdominal pain
Associated with weakness and giddiness.
He also complained of severe weight loss. He was 86 kgs 6 months ago but at present he reduced to 67 kgs.
He also has history of depression for which he is attending psychiatric counselling sessions.
Daily routine: He wakes up at 6am in the morning , gets ready and have breakfast ,go to the office ,completes his work and returns by 5pm and plays badminton or football and then comes to home ,have dinner at 8pm and goes to bed by 10pm.
PAST HISTORY:
History of trauma to nose in childhood while playing football and is having deviated nasal septum to left side which is not affecting his respiration
Episode of jaundice when he was 12 yrs old
Not a known case of DM, HTN,asthma,TB,epilepsy
History of appendicectomy when he was 17 yrs old
FAMILY HISTORY: No significant family history.
PERSONAL HISTORY:
DIET- Mixed
APPETITE- Normal.
SLEEP- inadequate
BOWEL AND BLADDER Regular
ADDICTIONS-
ALCOHOL- 180 ml every day since 20years .He had stopped consuming alcohol from 6 months because it increases the severity of abdominal pain.
SMOKING- 2 packs a day when he was in college. 1 pack a day from 6 months.
ALLERGIES- no allergies
GENERAL EXAMINATION:
Patient was conscious , coherent ,cooperative
moderately built and nourished
Vitals:
Temperature - Afebrile
PR :- 80 bpm
RR :-16 cpm
BP :- 110/70 mm Hg
SPO2 :- 98%
Pallor: present
Icterus: absent
Cyanosis: absent
Clubbing: absent
Generalised Lymphadenopathy:absent
Pedal edema:Absent
SYSTEMIC EXAMINATION:
CVS-S1, S2 heard,no murmurs
Respiratory System:-
BAE- present
NVBS- heard
Per abdomen:-
soft , non tender.
CNS- no focal neurological deficits






PROVISIONAL DIAGNOSIS
Chronic pancreatitis secondary to alcoholism
INVESTIGATIONS
Hemogram
Hemoglobin 11.2g/dl
RBC count 4.27 million/mm3
Platelets 2lakhs /mm3
Total count 4700/mm3
Eosinophils 02%
Basophils 00
Neutrophils 64%
Monocytes 02%
Lymphocytes 22%
Liver function tests
Total bilirubin 1.53mg/dl
direct bilirubin 0.25 mg/dl
SGOT 42 IU/L
SGPT 72 IU/L
Alkaline phosphatase 1242 IU/L
Total protein 5.8g/dl
Albumin 2.9g/dl
A/G ratio 1.28
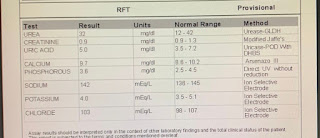
Renla function tests
Urea 25 mg/dl
Urice acid 4.5 mg/dl
Creatinine 0.9mg/dl
Serum electrolyte
Sodium 136 mEq/L
Phosphorus 3 mg/l
Potassium 3 .6 mEq/l
Calcium9.2 mg/l
Serum Amylase 172 IU/L Normal 25 to 140 IU/L
Serum Lipase 72 IU/L Normal 13 to 60 IU/L
CT scan Abdomen
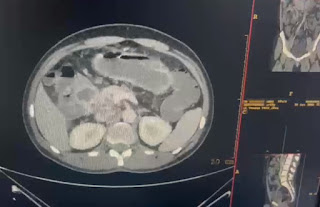
Findings
Bulky head and uncinate process of pancreas with heterogeneous cystic areas within with surrounding mild fat stranding and fluid.Small calcific focus along anterior surface of body of pancreas.Thin pancreatic body and tail with mildly dilated main pancreatic duct
Treatment
Inj. Tramadol 1 amp in 100 ml NS OD
TAB. Thiamine 100mg BD
IV fluids NS , RL @ 75ml/hr
Tab. Pantop 40mg OD


Comments
Post a Comment