A 45 year old male with hypokalemia
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 45 year old male resident of cherlapally farmer by occupation came with complaints of pain in the right upper limb near the (shoulder)since 10 days
HOPI
Patient was apparently asymptomatic 2 yrs back.
Then his appetite increased for which he came to our hospital and diagnosed with Diabetes.
He used oral hypoglycemic agents for the first six months and from past one and half year he is on insulin
History of increased urine output since 2 years
History of weight loss(25 kgs) since 2 yrs
In August 2022 he developed slurring of speech for which he was admitted in our hospital and diagnosed as Urosepsis
Again in October she had shortness of breath for which he came to our hospital and 4 sessions of dialysis was done
Now since 10 days he had pain in the right upper limb and swelling in upper limb since 1 day
On 23 /11/2022 he came to our hospital with complaints of pain in the right upper limb since 10 days and swellingand discharge(serous) in upper limb since 1 day
No h/o fever vomiting loose stools
There is h/o difficult in getting up and his sleep is disturbed since 10 days
He was admitted in General surgery and diagnosed with gas gangrene for which Incision and drainage was done under local anaesthesia.
Now he is referred our department as the patient have metabolic acidosis and hypokalemia
DAILY ROUTINE
Wake up in the morning by 4am then he will have milk by 5am and then he eat food (rice)by8am and then he goes for cattle rearing come back by 3pm then he takes some food rest and then he takes food at 6pm and goes to sleep by 7pm
His daily routine disturb after he developed the illness
PAST HISTORY
No similar complaints in the past
No history of hypertension Asthma Tuberculosis
Personal history
Diet:mixed
Appetite: increased
Sleep: disturbed
Bowel (loose stools)and bladder(irregular)
Addictions: Alcohol since 25 yrs (180ml/day)
FAMILY HISTORY:No significant family history
DRUG HISTORY:No history of allergy to any drugs
GENERAL EXAMINATION
Patient was conscious coherent and cooperative
Poorly built and nourished
Pallor present
No Icterus
No cyanosis
No clubbing
No generalized lymphadenopathy
Bilateral pedal edema present
Vitals
Temp Afebrile
PR70 bpm
BP 130/70 mm Hg
RR 16 cpm
GRBS 102mg/dl on 30/11/2022








SYSTEMIC EXAMINATION
Respiratory System
Inspection
Symmetrical chest seen
No scars and sinuses
Trachea is Central in position
Palpation:
Inspectory findings are confirmed
Expansion of chest is equal in all planes
Percussion:
Resonant note present over all lung areas
Ascultation:
Normal vesicular Breath sounds heard.
PER ABDOMEN
Inspection:
Abdomen is flat
No Abdominal distension
No scars, sinuses, mass visible
No engorged veins are seen
Umbilicus is central and inverted
No visible pulsations
Movements are equal over 9 regions during respiration
Palpation:
All inspectory findings are confirmed
No local rise of temperature
No Tenderness
No hepatomegaly and No spleenomegaly
Percussion
Normal
Auscultation
: Normal bowel sounds heard
No bruit heard
CARDIOVASCULAR SYSTEM EXAMINATION
Inspection : Bilaterally symmetrical chest present
No scars, sinuses
Palpation:
Inspectory findings are confirmed
Apex beat normal
On Auscultation :
S1 S2 heard
No murmurs or additional heart sounds
CENTRAL NERVOUS SYSTEM EXAMINATION
No focal neurological defecits
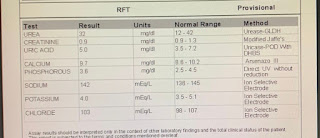
INVESTIGATIONS
On 23/11/2022













ECG


PROVISIONAL DIAGNOSIS
Right upper limb gas gangrene (post op) with hypokalemia
TREATMENT
On 1/12/2022
I.MVT 500 ml OD IV
I.meropenem IV BD
I.Clindamycin IV TID
I.Astymin IV BD
Tab Pantop 40 mg peroral OD
T.Nodosis500 PO OD
.T.Chymoral peroral OD
T.Dolo 650 PO OD
Syrup.Potklor PO OD
Protein Powder in 1 glass of water
T.Orofer PO OD
T.Vit c PO OD


Comments
Post a Comment