A 55 yr old female with fever and yellowish discoloration of eyes
A 55yr old female resident of thondlai came with chief complaints of fever , yellowish discoloration of eyes since 20 days.
generalized weakness and dizziness 3 days .
HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic 20 days back and then she developed fever which was intermittent (4 or 5 times since 20 days) and evening rise of temperature was seen for which she took paracetamol and it subsided .fever was not associated with chills and rigors.
She also had yellowish discoloration of eyes and urine since 20 days .
She also complains of burning micturition.
she came to our hospital on and was asked to get admitted but due to financial problems their family denied it.
Treatment advised was- tab Udiliv 300mg BD,
Tab Dolo 650mg sos, continue antihypertensive and anti diabetic medications.
And then she took herbal medicines every monday for 2 weeks and stopped anti diabetic and anti hypertensive medications completely since 1 week(when she started taking herbal medications)
Since 3 days she had generalized weakness and dizziness for which again she came to our hospital.
Patients daily routine
Gets up at around 6 am and does house hold work and stays at home all the day. she will have break fast around 9 am and lunch at 1 PM and dinner at 8 pm And sleeps around 9 pm .
She stopped doing any work since 20 days
PAST HISTORY
History of diabetes and hypertension since 5 yrs
No history of TB asthma epilepsy , chronic disease
FAMILY HISTORY
No significant family history
PERSONAL HISTORY
Diet: mixed
Appetite normal
Sleep adequate
Bowel and bladder regular
Addictions alcohol occasionally
TREATMENT HISTORY
Using Amlodipine for hypertension
And glimiperide, metformin for diabetes
Since 5 years
GENERAL EXAMINATION
Patient is conscious, coherent and cooperative.
Well oriented to time place person
Moderately built and moderately nourished
No pallor
Icterus present
No cyanosis
No clubbing
No generalised lymphadenopathy
No edema
VITALS
PR: 80bpm
RR: 16cpm
TEMP :Afebrile
BP: 140/90mmhg
SP02 :99%
SYSTEMIC EXAMINATION
RS: Bilateral air entry present
Normal vesicular breath sounds heard
CVS : S1 S2 heard, no murmurs
CNS: No focal neurological deficit
PA:
No abdominal distension
No tenderness
Umbilicus- normal
Movements -moves with respiration
No sinuses, distended veins
Scar of hysterectomy 20yrs back
No palpable mass
Liver is palpable
Spleen is not palpable
Bowel sounds heard




INVESTIGATIONS
Hemogram
Hemoglobin 12.7/dl
RBC count 4.27 million/mm3
Platelets 2.07/mm3
Total count 10000/mm3
Eosinophils 04%
Basophils 00
Neutrophils 58%
Monocytes 10
Lymphocytes 28
PCV 38 vol %
MCV 90.4 fl
MCHC 30 %
MCH 30 pg
Liver function tests
Direct bilirubin 15.9mg/dl
Indirect bilirubin 10.9mg/dl
SGOT 1172IU/L
SGPT 795 IU/L
Alkaline phosphatase 456IU/L
Total protein 6.9g/dl
Albumin 3.55g/dl
A/G ratio 1.06
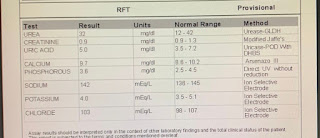
Serum electrolytes
Sodium 138mEq/L
Potassium 4 mEq/L
Chloride 102 mEq/L
Blood urea 20 mg /dl
Serum creatinine 0.6mg/dl
HbsAg Rapid Negative
Anti-HCV antibodies Non reactive
Complete Urine Examination
Colour pale yellow
Appearance clear
Reaction Acidic
Specific gravity -1.010
Albumin Nil
Sugar Nil
Bile salts Nil
Bile pigments
Pu s cells 1-2
Epithelial cells 2-3
Red blood cells Nil
Crystals Nil
Casts Nil
Amorphic deposit Nil


TOXIN INDUCED HEPATITIS
TREATMENT
1. Inj Pantop 40mg OD IV
2. Inj Zofer 4mg IV
3. Inj Neomol 1gm IV
4. Tab PCM 500mg BD
5. Tab Rifagut 550mg
6. Inj Trenexa 500mg IV stat
7. Tab Udiliv 300mg BD
8. Syrup Lactulose
9. Syrup Aristrozyme 25ml TID
10. Protein rich diet
11. Temperature charting ,GRBS monitoring .


Comments
Post a Comment