A 65 old female came with chief complaints of decreased appetite since 10 days
A 65 year old female came with chief complaints of decreased appetite,fever , generalised weakness and irregular bowel and bladder since 10 days.
HOPI
Patient was apparently asymptomatic 5 yrs back.
Then she was diagnosed with diabetes mellitus and hypertension when she went to the hospital for the general check up.
She is on medication for HTN and stopped using medication for DM since year because of the low sugar levels
Then 1 year ago she developed swelling of legs for which she went to the hospital and she was told the kidney is shrunken and she has infection in the kidney.she used mediation for this problem.
Now since 10 days her appetite was decreased and she also had fever which was high grade and more during the night time and associated with chills and rigor.
She also had history of vomiting since 10 days like 1 episode per day
Bowel and bladder was irregular but since 2 days it became regular because she took a tablet.
Her daughter complained of weight loss also
Patient s daily routine
Patient was a agricultural labourer but stopped working since 1 year because of weakness.Now she gets up in the morning and does some personal work and leading a sedentary life.
PAST HISTORY
No similar complaints in the past
History of DM and HTN since 5 years.No history of TB, Asthma, Epilepsy
Treatment history:Telmisartan for HTN
PERSONAL HISTORY
Diet Mixed
Appetite decreased
Bowel and bladder regular
Sleep adequate
No addictions
FAMILY HISTORY
No significant family history
GENERAL EXAMINATION
Patient was conscious coherent and uncooperative
Moderately built and nourished
Pallor: present
Icterus absent
Cyanosis absent
Clubbing absent
Generalised lymphadenopathy absent
Edema absent
Vitals
Temperature Afebrile
RR 19 cpm
PR 74 bpm
BP 140/90 mm Hg
Systemic examination
Respiratory system BAE present , normal vesicular breath sounds heard
CVS s1,s2 heard, no murmurs
GIT soft and non tender
CNS No focal neurological deficit



INVESTIGATIONS













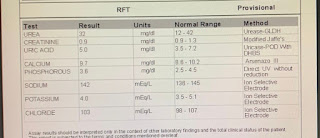
RFT
Urea 96 mg/dl
Creatinine 2.3 mg/dl
CBP
Haemoglobin 6.3
PCV 18.3
RBC 2.3 million/mm³
Provisional diagnosis
TREATMENT
Inj Neomol 100 ml/IV/
Inj PAN 40 mg/IV/OD
Inj Zofer 4g Iv(SOS)
Inj OPTINEURON 1 amp in 100 ml NS/IV/OD
Tab ECOSPIRIN AV (75/20) po/Hs


Comments
Post a Comment